
Showing Their Buts: the False Compassion of the Concerned
“Compassion is important, but,” a beautiful turn of phrase that calls to mind the immortal words of the great leader Eddard Stark. Everything before the word "but" is horseshit.


Some moderates seem to really like saying they think progressives should compromise on certain elements of trans rights. Op-eds and interviews of this type tend to paint some aspects of the movement as irrational and extreme while endlessly providing reasonable-sounding paraphrases of its opponents. To achieve this, pundits and politicians make sure to take up a stance of compassionate, reluctant resignation to the supposed “reality” that some trans rights are either unattainable or unreasonable.
This approach is sold at times as a principled commitment to weighing the rights of one group against perceived harms to another, at other times as a call to electoral pragmatism, and at others as a criticism of the so-called “intolerance” in the progressive movement toward centrist views. All these framings obscure and even contradict important acts about how and whether we should make the case for the rights of a group that is under attack, so after isolating these three primary themes I decided to look into the discursive strategies, positioning, and ideologies associated with the first theme: some trans rights jeopardize the rights of others.
“Compassion is important, but”
It’s a fine line to walk, maintaining a posture of compassion toward the trans rights movement while also arguing that some of their demands are a bridge too far, but this nation’s greatest centrists are more than up to the challenge.
In a March 2025 essay for Persuasion titled “How to Navigate Transgender Issues in the Trump Era,” Cathy Young expertly threads the needle by asserting that “Compassion is important, but,” a beautiful turn of phrase that calls to mind the immortal words of the great leader Eddard Stark.

After the “but,” the reader is treated to a list of people Young believes are harmed when we show too much compassion to trans people. We actually get to see this argument’s “but” a few times. For example, the second paragraph goes:
The idea of sacrificing a minority’s civil rights for political gain is rightly seen as repugnant, and there is no question that the Republican Party is currently engaged in some disgraceful assaults, in words and action, on transgender Americans. But it is also important to acknowledge that some of the issues implicated in this debate are not straightforward matters of civil rights; that concerns about progressive overreach are not simply a right-wing culture war panic; and that such concerns also relate to important questions about harm to the vulnerable.
In the Atlantic, Jonathan Chait shows us his “but,” too. To the “major questions about trans rights,” he proudly proclaims, “I believe the moral answer to all of these questions is a clear yes,” but Democrats suffered because “they either supported or refused to condemn a few highly unpopular positions: allowing athletes who transitioned from male to female to participate in high-level female sports, where they often enjoy clear physical advantages, allowing adolescent and preadolescent children to medically transition without adequate diagnosis; and providing state-funded sex-change surgery for prisoners and detainees.”
California Governor Gavin Newsom’s “but” is mostly interested in sports. He apparently wanted everyone to see his “but” so badly, he dedicated a significant portion of his first podcast episode to showing it to Charlie Kirk. “I’ve been a leader in the LGBTQ places, as you know back in 2004 [I] was marrying same sex couples,” he reminds us, before agreeing with Kirk that trans girls shouldn’t be competing against cis girls in sports. “I take a backseat to no one….But the issue of fairness is completely legit. So I completely align with you, and we’ve got to own that, we’ve got to acknowledge it.”
Matt Yglesias’s “but” has thoughts about science. In his Substack, which is read by top Democratic members, he writes that “trans rights is a niche issue that directly impacts few people” but “the general fact that there are men and women and they are (on average) different is a salient and important feature of human society.” In his estimation, “Americans, as free and equal human beings entitled to respect and dignity, should not be forced to live within the shackles of traditional gender norms if they don’t want to. But it doesn’t work for a major political movement to pretend not to see what’s plainly visible.” Apparently “bad science” is to blame for the belief that there are cases where it’s perfectly fair for trans girls and women to play sports with cis girls and women.
These “buts” serve to imply that some trans rights would come at the risk of causing “harm to the vulnerable” or, in Yglesias’s words, result from progressives being “uncomfortable with the fact that men and women are different.” It’s effective because nobody wants to harm the vulnerable or advocate against the facts. In Albert O. Hirschman’s the Rhetoric of Reaction, this is the thesis of “jeopardy,” a reactionary way of stonewalling that cuts off debate by sidestepping the question of whether the proposed social change is right or necessary, shifting focus to progress made in the past and suggesting that it will be destroyed. The specific rights that are named as too dangerous differ slightly, but the ones most commonly named just so happen to be the rights most viciously attacked by the extreme right. They are women’s sports, transgender children, and medical transition for prisoners.
Women’s sports
In the wake of the 2024 presidential election, Democratic politicians opined that trans women’s participation in sports was a significant problem for the party because they’d committed to a policy that was morally wrong. Representative Tom Suozzi from New York told the New York Times, “I don’t want to discriminate against anybody, but I don’t think biological boys should be playing in girls’ sports.” Massachusetts Representative Seth Moulton gave a similar quote to a different set of New York Times reporters: “I have two little girls, I don’t want them getting run over on a playing field by a male or formerly male athlete.”
These politicians got way over their skis in wrongly implying that prepubescent trans girls should be considered different from their cis counterparts on the field, but most centrist pundits tend to be more restrained, focusing on teens and adults. To do this, they rely on the myth that an endogenous puberty has irreversible impacts on athletic performance.
In the context of sports, Young writes that “the clash between women’s rights and much transgender advocacy is obvious.” As evidence for this, Young links to two essays from the online magazine Quillette, one of which contains cruel insults about a minor’s appearance and details that don’t match the available information. The other is about college volleyball teams forfeiting games in protest against a trans player. Neither even pretends to show any evidence for actual sports advantages. She also joins Chait and other pundits in relitigating the case of swimmer Lia Thomas by way of a New York Times piece by Michael Powell.
There’s a reason the same handful of anecdotes keeps getting shared around instead of actual data. In order to argue that trans women who went through endogenous puberty can never compete fairly in women’s sports, one must misrepresent or entirely skip the part of that argument that would require referring to data or scientific studies on the matter. As it turns out, the natural advantage of trans women in athletics has been wildly overstated.
One way this happens is by comparing cisgender men to cisgender women and assuming without evidence that transgender women will perform like the men. This is the route Powell takes in his article, but he is not alone. In 2022 at CPAC, Donald Trump said of former college swimmer Riley Gaines, “I’m much bigger and much stronger than her. There’s no way she could beat me in swimming.” Yeah, and twelve percent of British men could totally beat Serena Williams at tennis.
Another way to exaggerate advantage is to compare trans women who are athletes to sedentary cisgender women. Both strategies will give a skewed view of the biological realities underpinning athletic performance and transition. Ultimately, the scientific literature is clear: once they have been on hormone replacement therapy for one to two years, athletic trans women perform the same or even less well when compared to athletic cisgender women. Because the trans rights centrists cannot justify excluding trans girls and women on the basis of performance, they must do one of two things, Either they rely on salient exemplars and inaccurate or irrelevant anecdotes, or they abstract away from athletic performance so we forget that’s what we were supposed to be debating. That means focusing on the sex an athlete was assigned as a newborn baby, or her chromosomes, or the gametes her body appears organized around producing. There is no logical justification to keep her out that applies to direct measurement of her body or ability.
Much of the “fairness” discourse expresses anxiety about children, especially adolescents. When we’re asked to think of the children, we’re encouraged to imagine ourselves as the parents of a cisgender little girl. We are meant to imagine her athletic dreams dashed as her place on the podium is snatched by some hulking stranger.
But this stranger is someone’s daughter too, a child herself. Her parents are usually not even mentioned, and we’re certainly not encouraged to think of ourselves as the people responsible for taking care of her, drying her tears or wrapping her in our loving arms as she suffers through the onslaught of naked hate directed at her because Megyn Kelly decided to rant to her millions of followers about how she “stole the place of” a cis girl, repeating her full name and school several times over grainy cell phone footage of her taking second place in a regional track meet. We are not encouraged to imagine attending our daughter’s high school track meet and registering the pain in her eyes when she realizes some other girls’ fathers wore special wristbands to protest her. We aren’t supposed to think about what we would say upon answering a tearful phone call from our nineteen-year-old daughter because a woman decided to make her the new object of hate for every FOX viewer for weeks on end as punishment for the crime of fencing in a regional open after an executive order got her taken off her college team.

We certainly aren’t meant to wonder how we will handle ourselves if a stranger storms across the field to scream that our cisgender daughter doesn’t belong, calling us “groomers” and “child mutilators” because she has short hair.
To compromise on the question of girls and women’s sports would be to move away from the recommendations of experts, ignore what we know about sports science, and move toward a policy that isolates trans people from their peers and deprives them of healthy activities. There were already evidence-based regulations in place; replacing them with a blanket ban is not reasonable and sacrifices democratic values of fairness and equality.
Trans and gender-diverse youths
With some exceptions, the moderate voices in this conversation tend not to condemn youth social transition (trying out different names, pronouns, hairstyles, clothes, and other non-hormonal, non-surgical changes). In 2024, Gavin Newsom signed a bill into law prohibiting schools from firing teachers if they know something about a child’s sexual or gender identity and don’t tell the parents. It allows teachers to use discretion if they suspect someone at home will abuse the child or put them in conversion therapy, both of which are real risks. Echoing the words of Republican officials, his podcast guest Charlie Kirk described it as “a law where school districts can’t even tell parents if their kids are trans.” Newsom immediately corrected the mischaracterization and reaffirmed his support for the law. Kirk did not concede the point, pivoting instead to claiming the position was unpopular, but Newsom stood his ground again, saying, “I don’t mind losing, sometimes you lose on principle.”
But when it came to youth gender medicine, Kirk dominated the floor with a fast-paced screed: he called it “chemical castration of our kids” and said, “I encourage you, Governor, to learn about some of the butchery under the guise of healthcare in this state and in other states.” Newsom was either not able to cut in or had nothing to say, so Kirk went on unimpeded. After pivoting yet again to the question of popularity, he asserted, “There is no good counter to it … the United Kingdom Cass Report, the NHS came out and said there is no good reason to ever operate surgically on a young person. Puberty is not the problem, puberty is the solution.” Newsom barely had time to mutter, “I’m not an expert in this but I appreciate your broader—” before being interrupted again. The Cass report is an independent review commissioned by the British government that expresses reservations about the current standards of youth gender medicine. Sonia Sodha, a self-described “rational liberal,” celebrated that the Cass Report means “evidence not ideology will be used to guide children seeking gender advice.” Experts disagree vehemently.
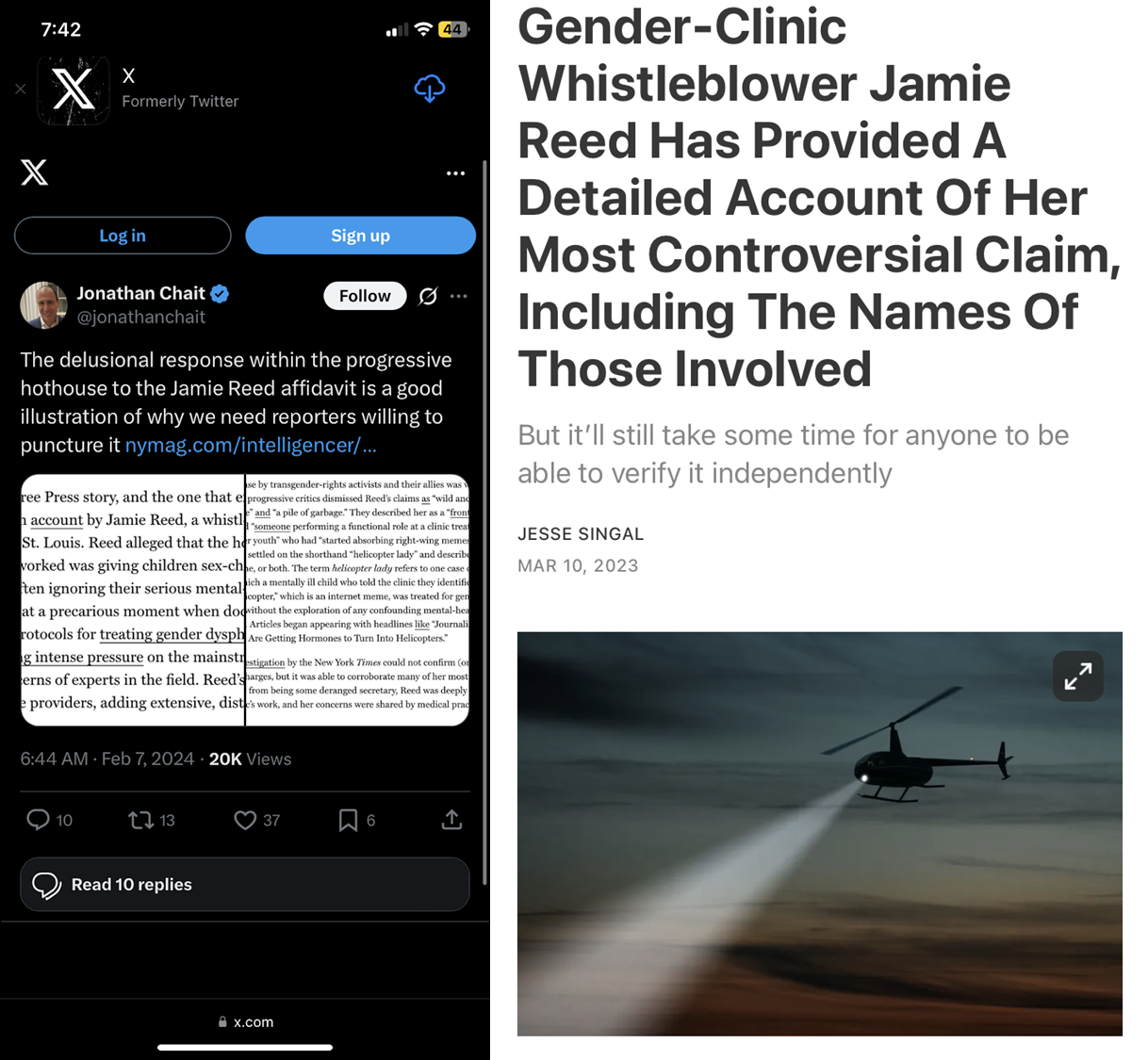
In the case of what Young calls “gender-distressed” youths, the compassionate but reluctantly unsupportive moderate must rely on “reports of gender-dysphoric children being rushed into hormone therapy and other interventions without adequate mental health safeguards.” She assures us that these “reports … have been confirmed by reporting.” But what is linked is the false claims of a “whistleblower,” a former employee at a gender clinic in St. Louis. After an eight-week investigation, it was determined that there were no instances of patients being rushed into treatment without appropriate assessment. This has been public knowledge for three years now, but somehow it has not made it across the desk of any of these professional concern-havers.
Since this wild rush isn’t actually happening (only about 0.0021%—that’s 2.1 in 100,000—of trans teenagers get any surgery at all, a significantly lower rate than cisgender youths receiving the exact same procedures), the concerned centrists have to figure out how to get us to feel panicky about the situation without robust evidence. They tend to construct what philosopher David Harker calls “created scientific controversies.” In the cases of cigarette lobby, climate change denial, creationism, anti-vaccine movements and anti-GMO movements, “[c]reated scientific controversies emerge when expert communities are in broad agreement but the public perception is one of profound scientific uncertainty and doubt.”
In Chapter 6, Harker runs us through a baker’s dozen of informal fallacies that typically characterize “created scientific controversies.” When Young says “71 percent of all Americans (and more than half of Democrats) believe that puberty-blocking medications and hormone therapies should not be available to anyone under age 18,” and Chait says the sports and youth issues “poll horribly,” they are committing fallacy number six: appeal to the masses. If the public is wrong on a topic, it’s okay to put some effort into working to persuade them instead of ceding the ground after a little polling. When Young says, “In the United States, political polarization has gotten in the way of finding a reasonable middle ground,” she’s giving us number twelve: argument to moderation, in which you “assume that the truth must lie somewhere between the positions being defended by opposing sides.”
It’s always possible to find a handful of people with the right credentials who don’t mind being the voice of doubt in a created controversy. Harker writes, “as long as some scientists were willing to repeatedly dispute the connection between cigarettes and lung cancer—no matter who paid their salary—the public would hear that some scientists were convinced by the evidence and some were not.” To this end, Young points to Erica Anderson, a psychologist who has penned many op-eds and appeared on television to warn of a coming spike in youth transition regret rates. The spike has so far not materialized, but this doesn’t stop her from being a media darling in the genre of “concerned expert.” Chait name-drops her too, in service of the point that trans people are not in lockstep with trans rights organizations. The fact that Anderson is transgender herself is always at the forefront. Identity politics are illiberal except when we can use it to our advantage. Like many in this genre, the op-eds in question engage in generalization, anecdotal cherry-picking, and a total refusal to link to any scientific studies that might be relevant to youth gender healthcare. They also frequently take an uptick in youth requests to access hormone therapy as proof that the prescription of hormones is out of control.
Many of these concerns reflect a faulty understanding of “gender-affirming care.” It is a form of equivocation in which the authors exploit the semantic ambiguity of the word “affirming.” In the context of gender-affirming healthcare, the authors want us to imagine that a child walks into a clinic, says, “I’m trans,” and the staff all say, “If you say so!” and pump them full of gender drugs right away. Sodha’s article claims that trans healthcare practitioners “put young people on life-altering pathways based on little but professional hunch,” and that trans kids are being treated as “little projects for activists seeking validation for their own adult identities and belief systems.”
But the actual practitioners of gender-affirming healthcare understand it to mean something completely different. The president of the American Academy of Pediatrics responded to the New York Times article on the “Growing Divide on Youth Gender Medicine,” writing,
Critics of our policy often mischaracterize gender-affirming care as aggressively pushing medications or interventions. That is wrong. There are no predetermined treatments or timelines. Gender-affirming care begins with conversation, and it often goes no further than that. For many young people, having the space and time to explore their gender identity with the support of their loved ones and health care team is critical to their well-being. This health care approach integrates medical, mental health and social services, including resources and supports for parents and families.
It’s true: reviews of gender-affirming care models show that they explicitly avoid privileging any particular outcome for the patient.
The concern-havers rely on this false definition of affirmation in order to argue that the barriers to youth gender medicine are too low, that in Young’s words, healthcare providers think “cross-sex identification in children should be presumptively regarded as a sufficient basis for social and (in adolescents) medical transition.” They’re expressing concerns that clinicians are, in Chait’s words, “allowing adolescent and preadolescent children to medically transition without adequate diagnosis.” What, then, should happen to the youths that might want to transition? These compassionate compromisers say they don’t want anything draconian, they just want kids to experience a pressure-free, exploratory process where we could be sure that only the ones who are “really” trans end up taking hormones. The model that actually does this is the affirmative model, but they won't accept this.
So when parents are convinced to avoid affirmative care, they end up turning to crank “experts” who say they have created a model that fits the brief. Therapists like the staff at Therapy First, who say they will “respect client autonomy and do not impose our own beliefs, values, opinions, ideology, religion, or goals on clients.” But when you look into what they actually practice, it is indistinguishable from conversion therapy, a practice of trying to force children to stop being trans. Therapy First is one of many centers that function like a crisis pregnancy center: keep the patient in sessions until it’s too late for puberty blockers.
So what does the scientific literature actually say about gender-affirming care and trans youths? Here is just a small sample of what’s available for the curious op-ed author.
The preponderance of evidence suggests that kids are not being given puberty blockers too often, too early, or too easily. Trans children’s gender identity is just as deeply rooted as that of their cisgender peers. In a longitudinal study of Dutch children, 98% of the children prescribed puberty blockers at the start of puberty went on to pursue hormone therapy as adults, so there is not an epidemic of kids prescribed puberty blockers who grew up to regret it. In fact, a team of University of Washington psychologists conducted a longitudinal study of gender diverse children, during which they discovered that families whose children are expressing a transgender identity spend significant time assuring the kids that they do not need to transition to have behaviors or interests that align with opposite-gender stereotypes. Many families also spent some effort forbidding their children to identify as the opposite gender.
What is happening, however, is that trans kids are experiencing significant discrimination that makes their lives harder. According to the 2022 US Trans Survey of over 92,329 respondents,
[m]ore than three-quarters of adult respondents (80%) and nearly two-thirds of 16- and 17-year-old respondents (60%) who were out or perceived as transgender in K-12 experienced one or more form of mistreatment or negative experience, including verbal harassment, physical attacks, online bullying, being denied the ability to dress according to their gender identity/expression, teachers or staff refusing to use chosen name or pronouns, or being denied the use of restrooms or locker rooms matching their gender identity.
Gender-affirming care is safe and healthy for trans youths. The WPATH standards of care for trans and gender-diverse youth requires a long list of conditions be met before beginning any medical treatment, including a detailed discussion of risks and mitigating steps they can take. Social transition brings their depression and anxiety down significantly, and puberty blockers and hormones do too. These findings match the results of the US Trans Survey.
Ultimately, preventing youths from accessing gender-affirming care is child maltreatment, medical interventions are still quite hard to get, and conversion therapy practices remain prevalent despite being denounced by professional bodies.
But all of this careful research can be hand-waved away as ideologically poisoned. According to Young, the field is compromised because of “the politicization, and arguably corruption, of science.” They cannot seem to let go of the idea that cisgender children are falling victim to “rapid onset gender dysphoria,” an unevidenced, pseudoscientific theory that kids are being “seduced” by the idea of transitioning by their friends and online influencers. Biased and unethical research that purports to support their view is retracted “on flimsy pretexts.”
In an interview for PBS, Jonathan Haidt endorsed this idea, saying Rapid Onset Gender Dysphoria (ROGD) “happens in clusters of girls,” that it’s not like regular gender dysphoria because social media created a situation where “girls get sucked into these vortices and they take on each other’s purported mental illnesses.”
On Pod Save America, Bill Maher seemed to hold a similar position. He claimed that kids have gender dysphoria because they feel bad “and then they blame it on the thing that has been put in their mind way too much, that it may be because of ‘you’re in the wrong body,’” comparing the process to “entrapment,” which he defined as “when you suggest something to people that they weren’t ordinarily going to do.” These concerned moderates seem to think that you can influence someone into being trans, rather than that lowered stigma makes it easier for trans people to come out. He makes the argument that there’s a reasonable compromise here, that you can tell kids “it doesn’t always have to be” that we match the gender marker on our birth certificate, “but that’s a different mentality than they put in the minds of kids.”
Just as when they talk about sports, the concerned moderates tend to take on parental concern as their primary lens, asking the reader to imagine themselves as the parents of a little girl who has suddenly, incorrectly identified as a boy, a sweet little girl who has been given medication and booked a date for a double mastectomy without going to a therapist who would properly screen her. “Our daughters.” “Your child.”
Frequently, these narratives tend to assert that parents are seeing a loss of rights to raise their children. Laura Edwards-Leeper and Erica Anderson, the two experts that are most often cited in the concern-havers’ essays, will point to a “constituency of agitated parents who feel excluded” that is “growing rapidly” and then as proof of this growing constituency they only link to an anti-trans organization called Genspect, a group so extreme they advocate for bans on social or medical transition for anyone under twenty-five.
The shifting of focus from the rights of children to the rights of parents has a long and bloody history. It’s easy to pretend that believing kids belong to their parents is the same as “[r]ecognizing that parents bear primary responsibility for their children's well-being.” In reality, “parental rights” are too frequently used to justify a refusal to live in a society where kids are allowed to attend racially integrated schools funded by the public where they will learn about history, evolution, and health science and how to get help if they experience sexual abuse, a society where they are protected from contracting preventable diseases and nobody is allowed to beat them, not even their own parents. There’s a reason the far right keeps accidentally quoting Hitler when they talk about how children should be treated: they don’t see them as full citizens who are entitled to bodily autonomy, self-determination, or even the opportunity to know inconvenient facts and think unauthorized thoughts.


It’s part of the “paranoid style” of radical conservatism: cosmopolitan elites are forcing themselves between you and your children, subverting the control over them you know you should be allowed to have and turning them into people who may not be perfect expressions of your expectations. It is not a framing that lends itself to healthy children, or healthy societies.
Again, when we are “thinking of the children,” we are supposed to imagine our child as cisgender, not as one of the trans and cis kids who would benefit from gender-affirming healthcare. We are not supposed to wonder how we would feel if our child, after consistently telling us he was a boy, being happier and more outgoing as a boy, was barreling towards an estrogen-fueled puberty that his doctors were not allowed to help him avoid. We are not supposed to imagine watching our little girl, having discussed with us and the medical staff all the possible side effects and risks, shrink into herself as she slowly realizes the gender health center we selected for her is staffed by people who never intended to refer her to an endocrinologist after all. And we are certainly not ever, ever supposed to imagine those kids as real people with rights and agency, to put ourselves in their shoes instead of the shoes of their parents. If we ever considered what it would have been like for us, as girls whose bodies were about to experience a flood of testosterone, or as boys with estrogen, how hard we would want responsible adults to fight for us.
We’re also not encouraged to think about the catch-22 this ideology creates for any trans girl who wants to follow her passion for sports: it is a bridge too far, according to these moderates, to offer her puberty blockers and prevent testosterone from conferring the physical advantages we are assured are a simple fact. But at the same time, once someone has gone through an endogenous puberty, nothing they can do will ever satisfy these same critics that she can compete fairly.
If we’re looking for things that actually harm children, there are real problems that politicians could focus on instead of banning youth gender medicine. 30% of parents in the US consider it appropriate to spank or hit their children despite the clear preponderance of evidence that it causes psychological and developmental damage. Child marriage is still legal in thirty-seven states: in 2018 nearly 2,500 children were married in the US that we know of. This is almost certainly an undercount. In 80% of those cases, the marriage rendered sex between the adult and their child spouse legal, thereby creating a “get out of jail free card” for what should be classed as statutory rape. Guns killed more than 2,500 children in 2022 and the rate is climbing. In 2023, about 374,000 children had less to eat than they needed because their household wasn’t getting enough food. Vaccine misinformation has allowed once-eradicated diseases to return, causing severe illness and even death to the children that catch them.
Youth transition is not only not dangerous, it’s necessary for the healthy and happy development of a subset of kids. That means it is important that we convince Americans and our legislators of the necessity of protecting it from repressive attacks.
Incarcerated trans people
In 2019, the American Civil Liberties Union sent the presidential and vice presidential candidates a questionnaire that included the question: “as President will you use your executive authority to ensure that transgender and nonbinary people who rely on the state for medical care—including those in prison and immigration detention—will have access to comprehensive treatment associated with gender transition, including all necessary surgical care,” to which Kamala Harris responded in the affirmative.

In fact, “yes” is the only reasonable answer to this question because the Eighth Amendment of the Constitution prohibits cruel and unusual punishment. After the supreme court case Estelle v. Gamble (1976), which held that the state must provide medical care for incarcerated people, a prison can be said to violate the Eighth Amendment if they (1) do not provide medically necessary care that is “reasonably commensurate with modern medical science” and (2) show “deliberate indifference” to the suffering caused by the lack of treatment. The standard of what is “medically necessary” would not be up to the President, so the answer has to be “yes” unless the respondent intends to knowingly violate the Constitution.
In 2024, the Trump campaign found that survey response and amplified it, spending over $200 million on ads attacking Harris over trans rights, more than they spent on housing, immigration, and the economy combined.
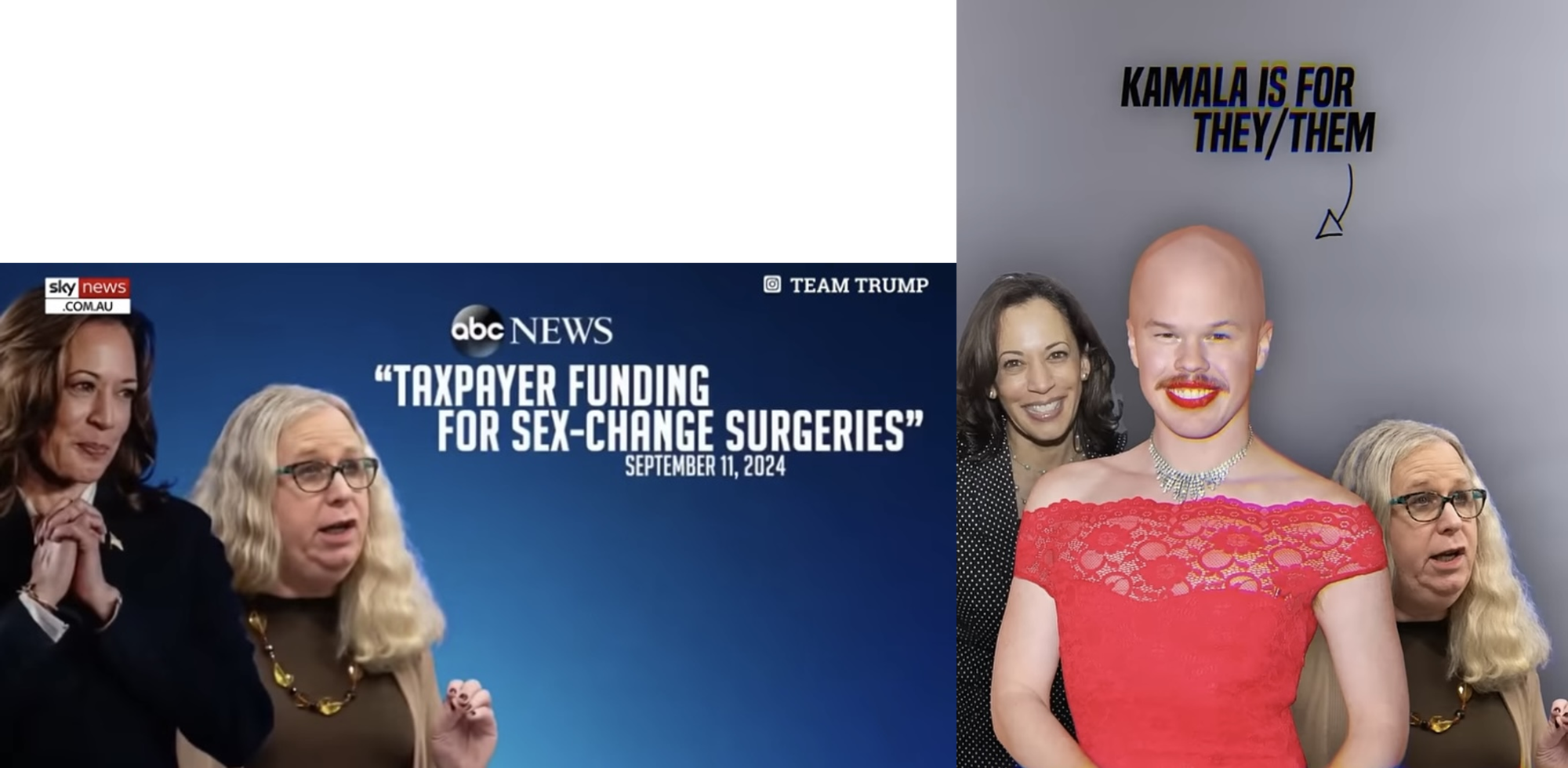
The text of the ads are about incarcerated trans people and kids playing sports, but most of the imagery was made of photos of Harris, Assistant HHS Secretary Dr. Rachel Levine (confirmed by Congress), and former deputy Assistant Secretary of Spent Fuel and Waste Disposition Sam Brinton (hired by Department of Energy and fired after they were convicted of luggage theft). Levine is a transgender woman and Brinton is gender-fluid. Despite not having worked in the administration for two years, Brinton’s photos are constantly being shared by the far right as evidence for how weird and gross the Democrats are. The subtext is clear: trans people’s mere existence in the government is intolerable.
Even though Harris’s answer was correct with respect to the law, democrats have expressed dismay at her position, implying the practice conflicts with our right to deny taxpayer funding for unpopular things. On Texas Public Radio,
[Texas Democratic Party chair] Gilberto Hinojosa said supporting transgender rights doesn’t necessarily have to include public funding for gender reassignment surgery. We can say, “OK, we respect people’s right to say, we don’t want my taxpayer money to be used for that.”
In his podcast episode with Charlie Kirk, Governor Newsom was emphatic and explicit in his disapproval. He called the ad “devastating” five times, lamenting that Harris “didn’t even react to it” and noting that “this was even more challenging because this issue was people who are incarcerated … individuals getting taxpayer-funded gender reassignment surgeries.”
It’s rare that an incarcerated transgender person needs surgery, and even rarer that someone has managed to fight through the bureaucratic and political obstacles to actually get it. In California, the state that processes the most requests, the policy cost under two million dollars for 2023, a drop in the bucket of the state corrections agency’s 15 billion dollar budget (notably, it was less than 1% of the budget for those Trump campaign ads). But even if it were expensive to provide this care, it would still be the responsibility of the American people and our government agencies to provide it. This is the legal and ethical mandate of the Eighth Amendment: when we imprison a person, preventing them from pursuing their healthcare independently, we must provide care as determined by experts to be medically necessary.
“Compassion, but” is a losing game
All this compassionate hand-wringing over sports and medical care for youths and incarcerated people reflects a gender anxiety that demands that we allow authoritarian ideologies about the body to stand in for facts about what is natural and essential. The illiberal biopolitics of gender are a vain effort to force a population to get in line behind an illusion: that men are fundamentally and irrevocably one kind of thing and women another, and that their job is to form nuclear family units for the production of more people who will be taught to play along to the same tune. By withholding opportunities to exercise the full range of rights that they should be entitled to, we force them into this mold, including by imposing our will on the development of their bodies. On opponents of youth transition, Samantha Hancox-Li writes, “They are trying to write their truth onto our flesh.”
Rather than commit fully to the out-and-proud fascist biopolitics of the Trump administration, the compassionate compromisers imply that there is a certain kind of trans person who can be afforded civil and human rights without endangering others. All they have to do is always be a perfect representative of their target gender but never give anyone cause to suspect that they are just appropriating gender stereotypes. They should get top and bottom surgery and never have experienced an endogenous puberty, but also not be “rushed into” youth gender healthcare (including the puberty blockers that would prevent said puberty). They must never rely on taxpayer-funded healthcare, never play competitive sports, never use any women’s facilities including in public bathrooms, spas, hospitals, homeless shelters, rape or domestic abuse shelters, and never commit a crime. Because those things all fall after the “but” in “Compassion is important, but.”
But if this is such a compassionate middle ground to take, if it is such a winning position for Democrats, why are extremists so eager to see Democrats take it on? On California Governor Gavin Newsom’s podcast, it was white nationalist extremist Charlie Kirk who took on the role of Democratic strategist, advising him, “You have an opportunity in this state to be like ‘Look, I have a heart for AB Hernandez, I have a heart for the San Jose volleyball player, let’s give them compassion, what’s not fair is just for like a women’s, entire women’s sports—’” to which Newsom interjected, “I agree. By the way, I agree with you. I agree with you.”
Asked what she thought about Moulton’s comments, Massachusetts Republican Party Chair Amy Carnevale told the Boston Globe, “Republicans agree that it’s entirely possible to respect gender preferences while also acknowledging that the physical differences between men and women create distinct risks in sports.”

The scorpion is asking for a ride. Surely we know better than to get anywhere near its “but.”
"Wild Animal Park" by andryone is licensed under CC BY 2.0.



